5. Correction of caudal strut deviation
To correct caudal strut deviation, it is essential to understand the removal of surplus cartilage, as previously emphasized in the context of septal growth. Techniques such as the batten graft, crosshatching/scoring incision are used to correct the deviation of the septal cartilage itself; however, merely addressing the cartilage deviation does not suffice for correcting the caudal strut. Instead, it is necessary to reposition the septum and correct any abnormalities at the junctions between the septal cartilage and surrounding structures. Methods that correct only the cartilage, like the batten graft, should be applied as secondary procedures, for instance, when reinforcing a weak caudal strut after correcting issues with the surrounding connections.
For caudal strut correction, procedures such as the swing door, door stop, and cutting and suture techniques can be utilized (Figures 1-9, 1-10).
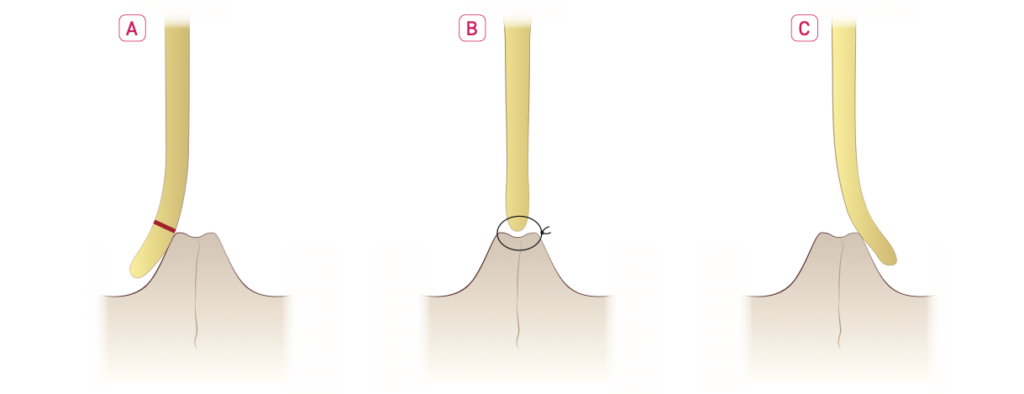
Figure 1-9. (A) Curved caudal strut: The red-marked area indicates the excess cartilage that needs to be removed. (B) Swing door technique: A portion of the excess cartilage is excised, and the remaining caudal strut is reattached to the anterior nasal spine (ANS). (C) Door stop technique: The excess cartilage is not removed; instead, the caudal strut is shifted to the opposite side of the ANS to correct the curvature.
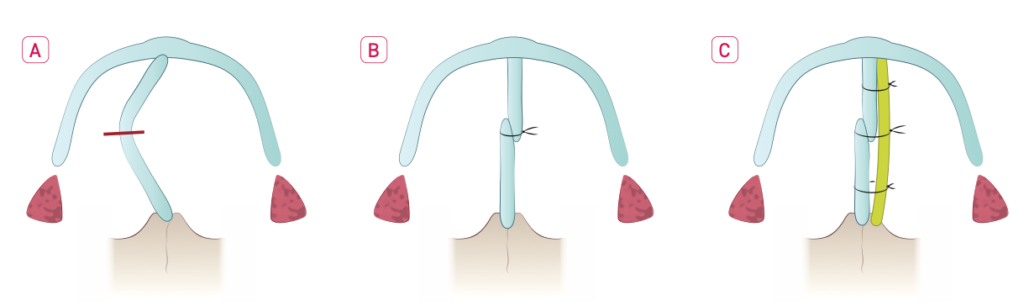
Figure 1-10. Cutting and suture technique: Without removing the excess cartilage or detaching it from the ANS, the caudal strut is cut, and the excess portion is overlapped and sutured together to correct the deviation.
The author primarily uses the swing door technique for correcting caudal strut deviation. This technique can be performed after harvesting all septal cartilage except for the L-strut in cases of rhinoplasty, though if septoplasty alone is being performed, any non-deviated portions of cartilage beyond the L-strut can be preserved. However, the maxillary crest, vomer, and adjacent septal cartilage should be partially trimmed to ensure full detachment from the bone (Figure 1-11). To execute the swing door or door stop techniques, a complete separation between the anterior nasal spine (ANS) and caudal strut is necessary (Figure 1-9). Following this, some surplus cartilage is excised and reattached to the ANS. Care must be taken to remove cartilage in thin layers, verifying alignment with the ANS after each excision to avoid excessive trimming. Once the proper amount has been excised, the caudal strut is reattached to the ANS, either by drilling a hole through the ANS or by securing it to the periosteum. To create a hole in the ANS, a drill can be used, although this may be cumbersome; applying pressure with tools like tower clips can create a passage large enough for a needle without a complete perforation. However, over-manipulating the ANS with clips may cause fractures, so cautiously using the clips as a guide for a vicryl 4-0 needle entry may suffice. As securing to the periosteum often provides adequate stability, drilling the ANS is recommended only when periosteal fixation proves insufficient.
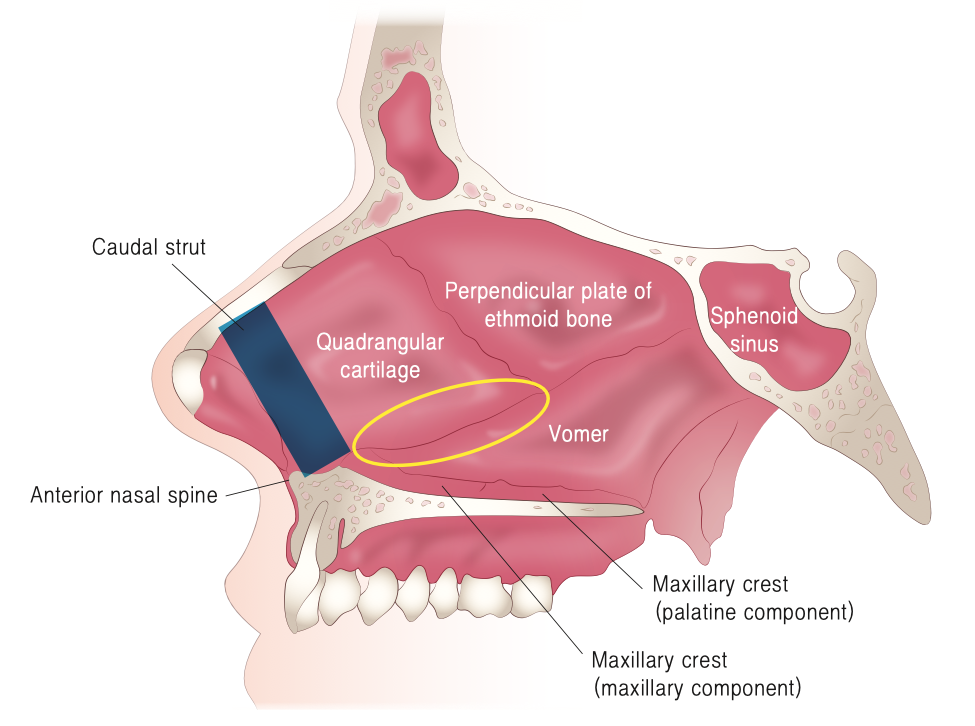
Fig 1-11. The area marked with a yellow circle is completely separated, and a portion of cartilage at the joint is excised. The deviated bony septum is trimmed to correct the deviation
Since firm suturing is needed in a confined space, multifilament sutures are preferred over monofilament ones. For instance, with a 4-0 suture, multifilament materials like vicryl 4-0 maintain the initial knot without loosening as easily as monofilament options such as PDS, facilitating stronger bonds.
The cutting and suture technique, which does not require separating the ANS from the caudal strut, may introduce unevenness at the overlap of the cartilage. While this unevenness can be an issue when adding a septal extension graft, making it a less preferred method for the author, it is a practical technique for standalone septoplasty (Figure 1-10).
In cases where the caudal strut is very weak, such as due to previous trauma or multiple rhinoplasty or septoplasty procedures, it is necessary not only to reinforce but potentially to reconstruct the caudal strut. Simple corrective techniques may be insufficient in these cases, so strengthening or recreating the caudal strut becomes essential. Reinforcement can involve using a harvested bony septum or remaining septal cartilage to perform a batten graft; however, in the author’s experience, this method does not provide adequate support along the entire length of the caudal strut and fails to create a strong attachment at the ANS (anterior nasal spine) if the caudal strut is weak. Therefore, using costal cartilage to create a new caudal strut is considered preferable.
To perform this procedure, the weakened caudal strut is fully detached from the ANS. Then, costal cartilage prepared as a new caudal strut is securely attached to the ANS. The original caudal strut is then firmly sutured to this costal cartilage, resulting in a robust neo-caudal strut that is firmly attached along its full length and provides a stable connection to the ANS (Figure 1-12).