6. Correction of high deviation
To explain the correction of dorsal strut deviation, it is essential to understand the keystone area and saddle nose. The keystone area is a specific region where the upper lateral cartilage (ULC) and nasal bone meet firmly. This area comprises the nasal bone, ULC, cartilaginous septum, and ethmoid perpendicular plate (Figure 1-13). Often, high deviation occurs due to deviation at the attachment between the ethmoid perpendicular plate and the dorsal strut. However, separating the bone-cartilage attachment in this area can lead to confusion with saddle nose.
As noted in discussions of septal development, the curvature in this region aligns with the growth direction of the bony nasal septum, so detachment from the bony septum is necessary. Proper removal of the curved bony nasal septum allows effective correction of high deviation. Additionally, if there is curvature at the connection between the ethmoid perpendicular plate and the dorsal strut in the keystone area, this section can be carefully separated. Correction of cartilage dorsal strut curvature requires relieving the tension from posterior bony deviation, making separation in this area essential for addressing high deviation.

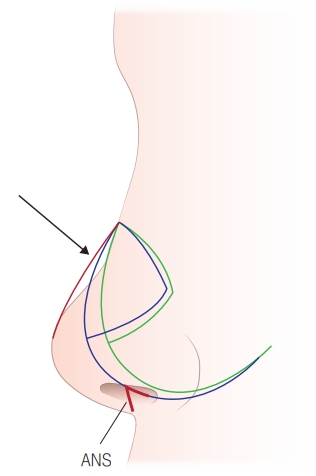
There is often a misconception that detaching the ethmoid perpendicular plate from the dorsal strut can cause saddle nose. This confusion arises from misunderstanding the attachment between the ethmoid perpendicular plate and the dorsal strut as the entire keystone area. In Figure 1-14, the black line represents a silhouette diagram of a saddle nose patient’s profile, showing how the nasal bridge should normally align like the red line. However, as indicated by the arrow, a section of the nasal bridge has collapsed, resulting in a saddle nose.
This saddle nose deformity is not caused by separating the attachment between the ethmoid perpendicular plate and the dorsal strut. Instead, it occurs when the septal cartilage, which should be positioned along the blue line before surgery, becomes separated from the anterior nasal spine (ANS) and shifts backward along the green line. This posterior displacement leads to the characteristic appearance of a saddle nose.
As previously mentioned, the keystone area is a specific region where the upper lateral cartilage (ULC) and nasal bone are firmly connected. This area forms a composite structure that includes the nasal bone, ULC, cartilaginous septum, and ethmoid perpendicular plate. Therefore, separating the attachment between the ethmoid perpendicular plate and the dorsal strut does not mean that the entire keystone area is detached. To correct high deviation, a selective dissection procedure should be performed in this area (Figure 1-15). Recent studies also support that detaching the attachment between the ethmoid perpendicular plate and the dorsal strut is essential for correcting cartilaginous high deviation (Kim et al., 2019).
Saddle nose typically occurs not from separation of the keystone area but rather when the septal cartilage shifts backward because the caudal strut and anterior nasal spine (ANS) were not resecured after detachment during surgery. To prevent this, care should be taken to avoid excessive retraction of the nasal speculum, which could cause detachment at the ANS attachment site. If detachment occurs, it is essential to reattach it, as described in caudal deviation correction, to prevent saddle nose.
Most high deviations arise from the attachment between the ethmoid perpendicular plate and the dorsal strut due to septal growth patterns. However, high deviation can also result from curvature within the cartilage dorsal strut itself. In these cases, a spreader graft can be used, similar to how a batten graft is applied in caudal deviation correction, to achieve a straightforward correction. If needed, the curved part of the dorsal strut can be resected, and a spreader graft can be placed to achieve proper alignment.