7. Correction of post-rhinoplasty septal deviation (correction of septal buckling)
During rhinoplasty, various manipulations are often performed on the septal cartilage. If only a columella strut is inserted without any manipulation of the septal cartilage, and if the issue, such as a posterior septal spur, is unrelated to the septoplasty surgical field or the rhinoplasty procedure, it can usually be corrected easily using conventional septoplasty techniques.
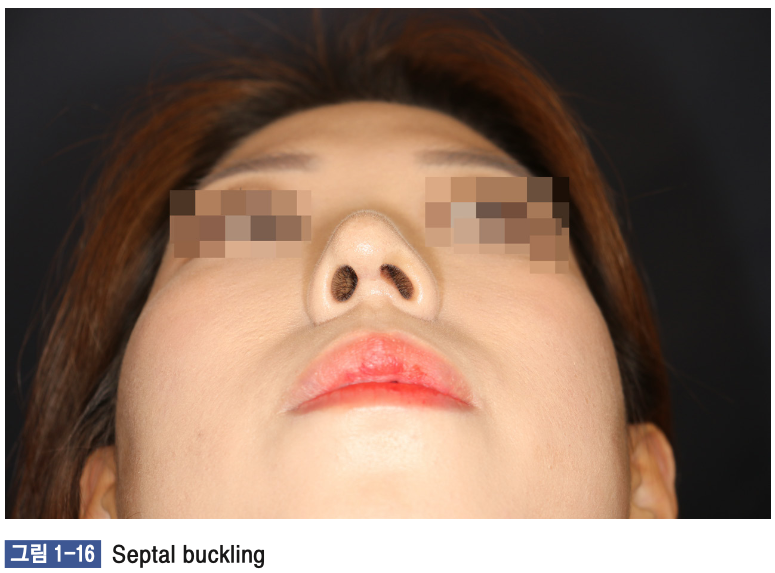
However, in most cases, nasal obstruction following rhinoplasty arises from the increased tension at the nasal tip. This tension applies pressure to the caudal strut via the expanded septal graft (SEG), resulting in caudal deviation. This deviation can extend to the columella, which is connected to the caudal strut through the SEG, causing columella deviation (as shown in Figure 1-16). Such cases are often referred to as septal buckling.
The aforementioned method for correcting caudal deviation can be applied, but it requires an open approach where the lower lateral cartilage is separated from the septal extension graft, the deviation is corrected, and the cosmetic aspects are then refined before concluding the procedure. However, if the patient is satisfied with their current nasal appearance and does not desire any cosmetic changes, a more efficient approach can be used.
This approach involves making incisions in the nasal mucosa on both sides, elevating the mucosal flaps, excising excess cartilage as per the principles of caudal strut correction, and reattaching the corrected structure to the anterior nasal spine (ANS). Since a septal extension graft is present, it is not possible to elevate the contralateral mucosal flap through a single incision, necessitating bilateral incisions. To prevent septal perforation, if any perforation occurs during the bilateral incision process, cartilage fragments should be inserted to avoid septal perforation (as shown in Figure 1-17).

8. The impact of septal cartilage and deviation on the external appearance of the nose.
he nasal septum is divided into a cartilaginous part and a bony part. It was previously explained that cartilaginous deviation can be corrected by separating it from the bony septum. This separation releases tension, allowing the position of the septal cartilage to change. The septal cartilage is connected superiorly to the upper lateral cartilage and inferiorly to the lower lateral cartilage via the membranous septum. Therefore, changes in the position of the septal cartilage can partially affect the positions of the upper and lower lateral cartilages.
For this reason, in cases where external nasal deviation is accompanied by septal cartilage deviation, correcting the deviated cartilaginous septum is an essential surgical procedure. Since the upper lateral cartilage is connected to the nasal bone, and the lower lateral cartilage is also attached to surrounding soft tissue, correcting only the septal cartilage is insufficient to completely correct the deviation of the cartilaginous nasal dorsum. However, correcting the deviation of the septal cartilage is a necessary step in addressing cartilage dorsum deviation.
Separately, the correction of the bony septum does not affect the external appearance of the nose. Unlike cartilage, bone is not an elastic tissue, so even if the entire deviated bony septum is removed, it does not cause changes in structures connected to the bony septum, such as the nasal bone.
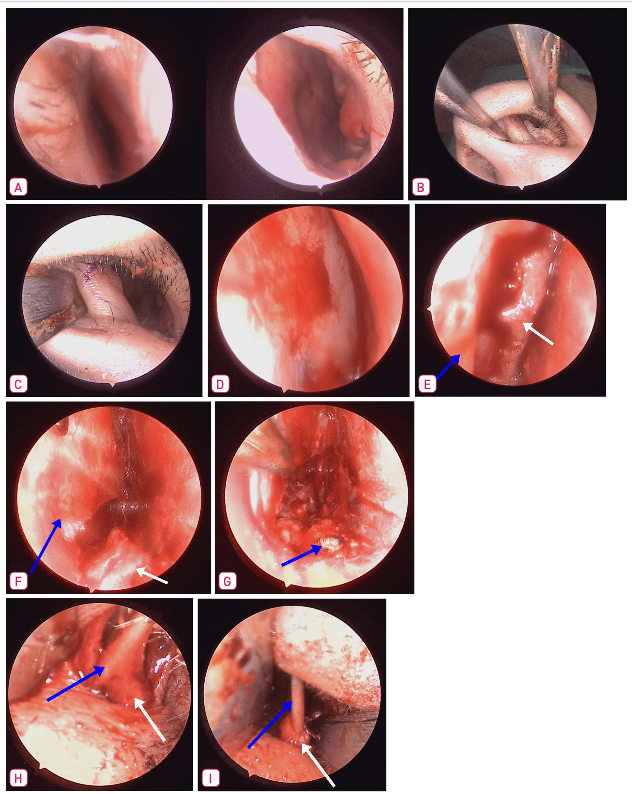
• (A) Preoperative condition showing Rt caudal deviation.
• (B) Visualization of the caudal end margin after spreading the nasal cavity.
• (C) Hemitransfixation incision line marked.
• (D) Subperichondrial mucosal flap elevation revealing a posterior Lt deviation in the high portion.
• (E) Separation of the bony septum and septal cartilage, with partial removal of the cartilage at the junction (white arrow: bony septum, blue arrow: septal cartilage).
• (F) Separation of the nasal crest from the cartilage, with partial resection of cartilage at the junction (white arrow: nasal crest, blue arrow: septal cartilage).
• (G) Resection of the nasal maxillary crest, with superior labial artery cauterized post-resection (blue arrow: maxillary crest).
• (H) Caudal strut displaced to the right of the ANS, showing deviation (white arrow: ANS, blue arrow: caudal septum).
• (I) After detaching the caudal strut from the ANS, trimming the excess cartilage and reattaching it to the ANS using a figure-of-8 suture (white arrow: ANS, blue arrow: caudal septum).